Meet Your California RN or LVN Continuing Education Requirements Quickly & Affordably.
Domestic Violence, Sexual Violence, Intimate Partner Violence - 3 Contact Hours
This course is approved through the California Board of Registered Nursing Provider #CEP 13509.
Course Outline
Outcomes
≥ 92% of participants will know how to identify and respond to domestic violence.
Objectives
After completing this course, the learner will be able to:
Define domestic abuse.
Identify 5 risk factors for violence against a spouse or significant other.
Define the cycle of violence and identify the key characteristics of abusers and victims.
Determine 3 reasons why victims stay with the abusive partners.
Categorize national and state mandates against domestic violence.
Summarize 3 reasons why victims of domestic violence are not identified in the healthcare system.
Formulate a plan to assess a victim of domestic violence.
Definition
Domestic violence amongst family members can take many forms. It may include emotional abuse, economic abuse, sexual abuse, threats, using the threat of removing children, isolation, and other behaviors used to maintain fear, intimidation, and power. Acts of domestic violence are categorized into psychological battering, physical battering, or sexual abuse (Centers for Disease Control and Prevention [CDC], 2020a).
While the term “domestic violence” is still widely used, more recently, physical, psychological, or sexual violence in a relationship is called intimate partner violence.
Physical Violence
When a person hurts or tries to hurt a partner by hitting, kicking, or using another type of physical force. The harm can range from bruises to death. It often begins more trivial and progressively escalates to more frequent and life-threatening attacks.
Sexual Violence
It is often broken into three categories:
Sexual activity that is compelled or forced.
Sexual activity with someone who cannot or is incapable of giving consent or understanding the sexual situation .Sexual activity that is abusive, degrading, or humiliating.
Stalking
Psychological Aggression
The use of verbal and non-verbal communication with the intent to harm another person mentally or emotionally, generally exerting control over another person.
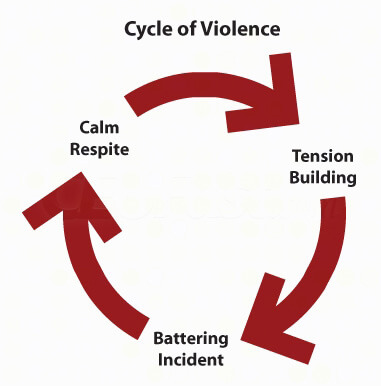
Cycle of Violence
Tension Building
Tension mounts in the relationship.
The batterer is irritable, frustrated, and unable to cope with everyday stresses.
The victim attempts to appease the batterer by becoming compliant, nurturing, or staying out of the way.
The victim often assumes responsibility for controlling the abuser's anger.
The victim denies the inevitability of the beating and the terror.
The batterer fears that the victim will leave and their fears are reinforced by the victim's coping strategy of withdrawing and avoiding.
The Battering Incident
The batterer generally intends to teach a lesson, not to inflict injury. In the process, they either lose control of their rage or act on their desire to exert domination or power.
Only the batterer can end this phase.
The victim needs a safe place during this phase.
Once over, the victim will deny the incident, injuries, and terror.
The Calm Respite of "the Honeymoon"
The batterer is kind and charming, afraid that the victim will leave.
The victim believes the suffering is over.
Then the cycle continues and returns to stage one.
Image 1: Cycle of Violence
Perpetrator
There are many theories as to why some people are abusers. However, abusers demonstrate the behavior they do because violence is an effective method for gaining and keeping control over another person. In a domestic situation, the abuser traditionally has not suffered adverse consequences due to violent behavior.
Abusers often display immaturity and are dependent and non-assertive (Sadock et al., 2021).
The psychological dynamics of male abusers include identification with an aggressor (father, boss, brother, etc.), testing behaviors (i.e., "Will she stay with me no matter what I do to her?"), distorted desires to express manhood, and dehumanization of women (Sadock et al., 2021).
Risk Factors
Family history of violence Alcohol and drug use - Emotional dependency, insecurity, and low self-esteem
Lack of impulse control - Antisocial, aggressive, and borderline personality disorders
- Poverty
- Marital discord or conflict
Triggers
Research from both developed and undeveloped countries has consistently identified the following triggers for domestic violence (DeCapua, 2017):
- Not obeying
Arguing back Not having food ready on time - Not caring adequately for the children or home
- Questioning about money or girlfriends
- Going somewhere without permission
- Refusing sex
The man suspects the woman of infidelity
Warning Signs
Batterers come from all social classes, races, cultures, religions, backgrounds, and countries (WHO, 2021). The following behaviors may be warning signs (DeCapua, 2017):
Extreme jealousy - Blames others for their faults and circumstances for their problems
- Unpredictable behavior
- Verbally abusive
Unable to control their anger - Always asking for a second chance, saying they'll change and won't do it again
- Their family resolves problems with violence
- It plays on your guilt
- Their way is the only way
- Behavior often worsens when using alcohol or drugs
- Cruelty to animals
Assessment Tool
Assessment tools have been developed that can help identify someone who has the potential for domestic violence/intimate partner violence.
Victims
Lack of Resources
- Responsibility for dependent children.
- Not employed outside of the home.
- The victim does not solely own any property.
- Lack of access to cash or bank accounts.
- Fear of being charged with desertion; therefore, losing children or joint assets.
- Fear of a decline in living standards for herself and her children.
Institutional Responses
- Clergy and secular counselors are often trained to see only the goal of saving the marriage at all costs.
- Police officers treat domestic violence as a dispute instead of a crime.
- Police may try to dissuade women from filing charges.
- Prosecutors are reluctant to prosecute cases and judges are lenient with the sentencing.
There is little to prevent a released abuser from returning and repeating the assault, even with a restraining order .There are not enough shelters to keep victims safe .
Traditional Ideology
The belief is that divorce is not a viable alternative .- The belief is that a single-parent family is unacceptable and that even a violent father is better than no father at all.
- Many women are socialized to believe that they are responsible for making their marriage work.
- The isolation of a victim contributes to a sense that there is nowhere to turn.
- Rationalization of their abuser's behavior by blaming stress, alcohol, problems at work, unemployment, or other factors.
Many women feel that their identity and worth are contingent upon getting and keeping a man .- During the non-violent phases, the abuser may fulfill the woman's dream of romantic love. She believes that he is good overall.
Males
Although women make up at least 85% of the victims of domestic violence, most often at the hand of male abusers, males are often victims (Kippert, 2021). In fact, according to the Centers for Disease Control and Prevention (2020), approximately 1 in 10 men in the United States have experienced sexual or physical violence and/or stalking by an intimate partner. Male survivors of abuse often experience a stigma to be the "man" who should have the ability to fight back against an abusive partner, especially when that significant other is a female (Kippert, 2021). In the case that the abuser is another male, they are often uncomfortable revealing the abuse because it would mean disclosing a same-sex relationship that they have not shared with others yet. Males also typically experience discrimination from police or domestic violence shelters (Kippert, 2021).
LGBTQ+ Community
Partner violence within the Lesbian Gay Bisexual Transgender Queer+ (LGBTQ+) community occurs quite often. Unfortunately, there is much less research available for this community in comparison to those in gender-conforming, heterosexual relationships (Resnick, 2021). The most current statistics from the National Coalition Against Domestic Violence (NCADV) state that 43.8% of lesbian women and 62.2% of bisexual women are raped, the victim of physical violence, and/or stalked by their partner (Resnick, 2021). The members of the LGBTQ+ community at the highest risk for intimate partner violence are African Americans, transgender persons, and bisexual people (Resnick, 2021).
The NCADV also stated that fewer than 5% of LGBTQ+ victims of domestic violence ever seek court-appointed protective orders (Resnick, 2021). Members of this community have their own unique reasons for not seeking help. First is the risk of potential discrimination from law enforcement. As mentioned in the last section, the abuser could threaten their partner if they have not "come out" to their family and friends to disclose a same-sex relationship. This threat can be potentially even more dangerous for any transgender, nonbinary, or those who are gender-nonconforming who have not publicly disclosed their gender identity (Resnick, 2021). In addition, homophobia and transphobia can still make a major impact in the legal proceedings of many states (Resnick, 2021).
Children
- Attention-deficit/hyperactivity disorder (ADHD)
- Anxiety
Behavioral problems, e.g., aggression - Depression
- Eating disorders
- Poor academic performance
- Low self-esteem
- Need for psychotropic medications
- Nightmares
- Physical health complaints
- Self-harming behaviors
Mandates Against Domestic Violence
The Joint Commission on Accreditation of Healthcare Organizations (JCAHO) defines standards for healthcare organizations and monitors compliance with those standards. JCAHO mandates that hospitals must develop criteria to identify possible victims of abuse.
Staff must be trained to apply these criteria. They should question whether abuse might have occurred if a patient's story for their injury does not match the actual injury. A hospital must maintain a list of private and public community agencies that provide help for abuse victims. Staff also must be able to make appropriate referrals for victims (DeCapua, 2017).
For example, a child's x-rays may show an unexplained broken bone. Staff should observe the behavior of the people who brought the child to the emergency room. Does the child cling to one parent and avoid the other? Staff members should question the child in a non-threatening manner, look for bruises on the body, and listen to explanations to see if there is congruence between the physical evidence and the story.
New York was the first state to require hospitals to establish protocols to identify and treat domestic violence victims and make referrals to community services. California passed the first state law mandating protocols for hospitals and clinics to detect the presence of violence in the lives of patients.
Governments and other donors should be encouraged to invest much more in research on violence by intimate partners over the next decade. Programs should place greater emphasis on enabling families, circles of friends, and community groups, including religious communities, to deal with the problem of partner violence. Programs on partner violence should be integrated with other programs, such as those tackling youth violence, teenage pregnancies, substance abuse, and other forms of family violence. Programs should focus more on the primary prevention of intimate partner violence.
Role of Healthcare Professionals
Early identification and intervention with victims of domestic violence can help prevent injuries and save lives (CDC, 2020b; U.S. Department of Health and Human Services, 2010). Many victims of domestic violence seek assistance in healthcare settings, often repeatedly, but are only treated for symptoms and injuries. Unfortunately, healthcare professionals often fail to identify victims. Missed cases of intimate partner violence may be due to the screening method.
Barriers to Thorough Screening
- Lack of time
Lack of training - Lack of resources
- Language barriers
- Cultural barriers
Emotional discomfort - Behavior of the victim, e.g., uncooperative, unwilling to accept help
Mental Health
Pregnancy
Pregnancy may be a risk factor for battering—approximately 1 in 12 women in North America who are pregnant, experience some form of intimate partner violence.
Violence during pregnancy increases the incidence of morbidity and mortality.
What We Can Do
Healthcare providers can help by screening for domestic violence, documenting abuse in the medical record, safeguarding evidence, providing medical advice, referrals, safety planning, and showing empathy and compassion.
Abuse victims need referrals to legal and social services. They may need help finding temporary shelter, advice on how to keep safe should they return home, and affirmation that the abuse is not their fault (DeCapua, 2017).
It is not the role of the healthcare provider to invoke or foster criminal justice intervention. Calling the police is not always in the best interest of a victim of domestic abuse. Some victims of domestic violence have learned to distrust the police or believe that law enforcement intervention will further endanger them. Immigrant victims may fear that calling the police will lead to deportation. Others are unwilling to use law enforcement intervention until a safety plan is in place.
Each victim should be informed of their legal options and encouraged to make their own choices (Cline et al., 2020).
Treating Victims of Domestic Violence
Identify patients who may be suffering from domestic violence. Encourage them to talk about it. Listen non-judgmentally. Validate their fears and concerns. Document their complaints, symptoms, and injuries. Assess the danger they are currently in. Provide appropriate referral and support .
The first step in treatment is the identification of the victim. Many individuals who are victims of abuse will not voluntarily share this information. However, they will discuss if the provider asks the right question in a compassionate, non-judgmental manner. The healthcare provider might start by asking, "Because violence is common in many people's lives, I ask every patient the same question. At any point, has your partner harmed or threatened you?" These conversations should always take place in a private setting when the patient is alone.
If the patient answers “yes” to this question, the healthcare provider should encourage them to talk about it and listen non-judgmentally. This talk helps begin the healing process and provides information that will help with treatment planning. It is also very important for the healthcare worker to validate the victim's fears because they often think others won't believe them or will downplay their experiences. The healthcare provider might say, "You don't deserve to be treated this way," and "You are not to blame."
The healthcare provider must document the patient's complaints and symptoms. The complaint should be written using the patient's own words and directly placed in quotations in documentation when possible. Also, be sure to detail and describe injuries, including their type, size, location, and number. If possible, take color photographs and include those in the chart as well.
Next, assess the danger to your patient. Determine whether they are safe to leave the healthcare setting. Indicators of escalating danger include an increase in the frequency, duration, or severity of assaults, new threats of homicide or suicide by the partner, threats to children or other loved ones, and the presence or availability of a gun.
Finally, healthcare providers should offer the appropriate referral and support. Start by treating the victims' injuries. If the victim is determined to be in imminent danger, refer them to stay with friends, family, or at a domestic violence shelter. If they are not in imminent danger, provide written information about community shelters and resources. Also, be sure to provide them with a toll-free domestic violence hotline number.
Case Study 1: Chelsea
Chelsea is a 43-year-old Caucasian female living with her second husband. She arrives at the clinic, appearing shaky and nervous. During the initial physical assessment, she begins to cry, explaining that her husband is aggressive. She describes his various behaviors, which could be classified as emotional, physical, and financial abuse. She has two children, ages three and six, who are both at the clinic with her.
She denies any current suicidal thoughts and any current drug or alcohol misuse. Assessment of the children does not reveal any evidence of abuse towards them, and Chelsea denies witnessing any aggression towards them in the past. The healthcare worker completes an assessment and explains to Chelsea her legal options. Chelsea agrees to go with her children to a local shelter to begin more specialized treatment and receive adequate community resources.
Case Study 2: Hamza
Hamza, a 28-year-old immigrant from Pakistan living in the Midwest, left his wife and moved into his friend's house after three instances of physical abuse. In addition, his wife was using financial control over him and isolating him from his family and friends. Hamza has obtained a restraining order, but his wife is attempting to retaliate by filing for a modification of custody for their children, citing frivolous allegations and inappropriate parenting. His lawyer represents him, and he has recently begun seeing a therapist for cognitive-behavioral therapy (CBT). This counseling has helped him emotionally process his situation and previous trauma.
Case Study 3: Christopher
Christopher, a 21-year-old college student, broke up with his violent boyfriend about a month ago; however, he continues to stalk him. He continues to show up on campus and will appear outside his classes, the cafeteria, and the library. He calls and sends him text messages daily, saying threatening and hurtful things. Christopher is scared and has been considering dropping out of school. He decides to seek help through a legal aid, who documents his stalking behavior and facilitates a meeting with the college dean. His attorney represents him in a court hearing and he can obtain a protective order to continue his education.
Conclusion
Domestic violence is a crime that causes severe health consequences. Healthcare professionals are mandated and obligated to identify and offer assistance to victims of domestic violence. Legal and societal changes in the United States have reduced the occurrence of domestic violence, but the problem is still an epidemic. Your efforts can make a difference.
Resources
National Hotlines
National Domestic Violence Hotline
- Staffed 24 hours a day by trained counselors who can provide crisis assistance and information about shelters, legal advocacy, health care centers, and counseling.
- 1-800-799-SAFE (7233)
- 1-800-787-3224 (TDD)
Rape, Abuse & Incest National Network
- The Rape, Abuse & Incest National Network (RAINN) is the nation's largest anti-sexual assault organization. Among its programs, RAINN created and operates the National Sexual Assault Hotline at 1.800.656.HOPE and the National Sexual Assault Online Hotline at rainn.org . This nationwide partnership of more than 1,100 local rape crisis centers provides victims of sexual assault with free, confidential services, 24 hours per day, 7 days per week. These hotlines have helped over 1.3 million people since RAINN's founding in 1994.
- 1-800-656-HOPE
State Coalitions on Domestic Violence
Alabama
Alabama Coalition Against Domestic Violence
- P.O. Box 4762, Montgomery, AL 36101
- Phone: 1-800-650-6522 (in state)
- Fax: 334-832-4803
- TTY: 1-800-787-3224
- Another State: 1-800-799-SAFE (7233)
- Email: info@acadv.org
- Crisis help lines are open 24 hours
Alaska
Alaska Network on Domestic Violence and Sexual Assault
- 130 Seward Street, Room 214, Juneau, AK 99801
- Phone: 907-586-3650
- FAX: 907-463-4493
- Hotline: 1-800-799-SAFE (7233)
- Email: lbrowne@andvsa.org
Arizona
Arizona Coalition Against Domestic Violence
- 301 E. Bethany Home Rd., Suite C194, Phoenix, AZ 85012
- Phone: 602-279-2900
- FAX: 602-279-2980
- TTY: 602-279-7270
- Toll-Free: 1-800-782-6400
- Email: info@acesdv.org
- Hours: 8:30am-5-00pm Monday - Friday
Arkansas
Arkansas Coalition Against Domestic Violence
- 1401 West Capitol Ave, Suite 170, Little Rock AR 72201
- Phone: (501) 907-5612
- FAX: (501)907-5618
- Toll-Free: (800)269-4668
California
California Partnership to End Domestic Violence
- PO Box 19005, Long Beach CA 90807
- Toll-Free: 888-SCCBW-52
- Phone: 916- 444-7163 562-981-1202
- Fax: 562-981-3202
- Email: jessica@cpedv.org
Coalition to End Family Violence
- 1030 N. Ventra Rd, Oxnard, CA 93030
- Phone: 805-983-6014
- FAX: 805-983-6240
- 24-Hour Hotline: 805-656-1111
- Spanish Hotline: 800-300-2181
- TDD: 805-656-4439
Colorado
- P.O. Box 503, Durango, CO 81302
- Phone: 970-247-9619 (24-hour hotline)
- Email: info@alternativehorizons.org
Colorado Coalition Against Domestic Violence
- 1120 Lincoln Street, Suite 900, Denver, CO 80203
- TOLL-FREE: 888-778-7091
- Phone: 303-831-9632
- FAX: 303-832-7067
- Email: ccadv@ccadv.org
Washington, DC
D.C. Coalition Against Domestic Violence
- 5 Thomas Circle, NW, Washington, DC 20005
- Phone: 202-299-1181
- FAX: 202-299-1193
- Email: info@dccadv.org
- Hours: 8:30am-5-00pm Monday - Friday
SOS Program (A part of DC Coalition)
- Domestic Violence Intake Center Satellite Office, Greater Southeast Community Hospital
- 1328 Southern Ave SE, Room 311, Washington, DC 20032
- Phone: 202-561-3095 x12
- Fax: 202-561-3093
- Hours: 9:00am-5:00pm
- P.O. Box 29596, Washington, DC 20017
- Phone: 202-529-5991 (24-hour hotline)
- Administrative Office: 202-529-5261
- Fax: 202-529-5984
Delaware
Delaware Coalition Against Domestic Violence
- 100 W. 10th Street Suite 703, Wilmington, DE 19801
- Phone: 302-658-2958
- FAX: 302-658-5049
- Hotline: 1-800-799-7233
- Email: dcadv@dcadv.org
Florida
Harbor House of Central Florida
- P.O. Box 680748, Orlando, FL 32868
- E-mail: contactus@harborhousefl.com
- FL Domestic Violence Hotline: 1-800-500-1119
Georgia
Georgia Advocates for Battered Women and Children
- 250 Georgia Avenue, S.E., Suite 308, Atlanta, GA 30312
- TOLL-FREE: 800-334-2836
- Phone: 404-524-3847
- FAX: 404-524-5959
Hawaii
Hawaii State Coalition Against Domestic Violence
- 716 Umi St., Unit 210, Honolulu, HI 96819
- Phone: 808-832-9316
- Fax: 808-841-6028
- Email: hscadv@pixi.com
24 Hr Hawaii Shelters by Island:
- Hilo: 959-8864
- Kauai: 245-8404
- Kona: 322-SAFE (7233)
- Maui/Lanai: 579-9581
- Molokai: 567-6888
- Oahu: 841-0822
Iowa
Iowa Coalition Against Domestic Violence
- 515 28th St, Suite 104, Des Moines, IA 50312
- TOLL-FREE: 800-942-0333
- Phone: 515-244-8028
- FAX: 515-244-7417
- E-mail: admin@icadv.org
Idaho
Idaho Coalition Against Sexual and Domestic Violence
- 300 E. Mallard Dr., Suite 130, Boise, ID 83706
- TOLL-FREE: 888-293-6118
- Phone: 208-384-0419
- FAX: 208-331-0687
- Email: jmatshushita@idvsa.org
Illinois
Illinois Coalition Against Domestic Violence
- 801 South 11th Street, Springfield, Illinois 62703
- Phone: 217-789-2830
- FAX: 217-789-1939
- TTY: 217-241-0376
- Email: ilcadv@springnet1.com
- (Formerly The Friends of Battered Women and Their Children)
- P. O. Box 608548, Chicago, IL 60660
- Phone: 773-274-5232
- FAX: 773-262-2543
- HOTLINE: 1-800-603-HELP
- Email: info@afriendsplace.org
- P.O. Box 1515, Des Plaines IL 60017
- 24-Hour Crisis Line: 847-824-4454
- Phone: 847-824-0382
- Fax: 847-824-5311
- Email: life-span@life-span.org
Indiana
Indiana Coalition Against Domestic Violence
- 1915 W. 18th Street, Suite B, Indianapolis, IN 46202
- TOLL-FREE: 800-538-3393
- Phone: 317-917-3685
- Fax 317-917-3695
- Crisis Line: 1-800-332-7385
Kansas
Kansas Coalition Against Sexual and Domestic Violence
- 634 SW Harrison, Topeka, KS 66603
- TOLL-FREE: 888-END-ABUSE (Kansas state-wide hotline)
- Phone: 785-232-9784
- FAX: 785-266-1874
Kentucky
Kentucky Domestic Violence Association
- P.O. Box 356, Frankfort, KY 40602
- Phone: 502-209-5382
- FAX: 502-226-5382
- Email: info@kdva.org
Louisiana
Louisiana Coalition Against Domestic Violence
- P.O. Box 77308, Baton Rouge, LA 70879-7308
- Phone: 225-752-1296
- FAX: 225-751-8927
- HOTLINE: 1-888-411-1333
Maine
Maine Coalition to End Domestic Violence
- 170 Park St., Bangor, ME 04401
- Phone: 207-941-1194
- FAX: 207-941-2327
- HOTLINE: 866-83-4HELP
- Email: info@mcedv.org
Maryland
Maryland Network Against Domestic Violence
- 6911 Laurel Bowie Road, Suite 309, Bowie, MD 20715
- TOLL-FREE: 800-MD-HELPS
- Phone: 301-352-4574
- FAX: 301-809-0422
- Email: info@mnadv.org
Massachusetts
Jane Doe Inc./Massachusetts Coalition Against Sexual Assault and Domestic Violence
- 14 Beacon Street, Suite 507, Boston, MA 02108
- Phone: 617-248-0922
- Crisis / Information: 989-686-4551
- FAX: 617-248-0902
- TTY/TDD: 617-263-2200
- Email: info@janedoe.org
Michigan
- P.O. Box 1458, 3411 E. Midland Rd., Bay City, MI 48706
- TOLL-FREE: 800-834-2098
- Phone: 517-686-4551
- FAX: 517-686-0906
- Michigan 24-Hour Crisis Line: 517-265-6776
Minnesota
Minnesota Coalition for Battered Women
- 590 Park Street North, Suite 410, St. Paul, MN 55103
- TOLL-FREE: 800-289-6177
- Phone: 651-646-6177
- FAX: 651-646-1527
- Email: mcbw@pclink.com
Missouri
Missouri Coalition Against Domestic Violence
- 217 Oscar Dr., Suite A, Jefferson City, MO 65101
- Phone: 573-634-4161
- FAX: 573-636-6613
Women's Support and Community Services
- 2165 Hampton Ave, St. Louis, MO 63139
- HOTLINE: 314-531-2003
- Office: 314-646-7500
- Hours: Monday-Thursday 8:00am-7:00pm; Friday 8:00am-1:00pm
Mississippi
Mississippi State Coalition Against Domestic Violence
- P.O. Box 4703, Jackson, MS 39296-4703
- HOTLINE: 800-898-3234
- After Hours HOTLINE: 1-800-799-7233
- Phone: 601-981-9196
- FAX: 601-981-2501
- Email: mcadv@misnet.com
- Hours: Monday-Friday 8:00am-5:00pm
- Crisis Line
- P.O. Box 6644, Great Falls, MT 59406
- Phone: 406-453-HELP
- TOLL-FREE: 1-888-587-0199
Montana
Montana Coalition Against Domestic and Sexual Violence
- PO Box 818, Helena MT 59624
- Phone: 406.443.7794
- TOLL-FREE: 888-404-7794
- Fax: 406.443.7818
Nebraska
Nebraska Domestic Violence and Sexual Assault Coalition
- 1000 "O" Street, Suite 102, Lincoln, NE 68508-2253
- TOLL-FREE: 800-876-6238
- Phone: 406-443-7794
- FAX: 406-443-7818
Nevada
Nevada Network Against Domestic Violence
- 220 S. Rock Blvd. Suite. 7, Reno, NV 89502
- TOLL-FREE: 800-500-1556
- Phone: 775-828-1115
- FAX: 775-828-9991
- 921 American Pacific Dr. Suite 300, Henderson, NV 89014
- Phone: 702-451-4203
- FAX: 702-451-4302
- HOTLINE: 702-564-3227
- Email: kareng@safehouse.org
New Hampshire
New Hampshire Coalition Against Domestic and Sexual Violence
- P.O. Box 353, Concord, NH 03302-0353
- TOLL-FREE For Domestic Violence: 866-644-3574
- TOLL-FREE For Sexual Assault: 1-800-277-5570
- Phone: 603-224-8893
- Fax: 603-228-6096
New Jersey
New Jersey Coalition for Battered Women
- 1670 Whitehorse/Hamilton Square Road, Trenton, NJ 08690
- TOLL-FREE: for Battered Lesbians: 800-224-0211 (in NJ only)
- Phone: 609-584-8107
- FAX: 609-584-9750
- HOTLINE: 1-800-572-7233
- TTY: 609-584-0027 (9am-5pm, then into message service)
- E-mail: info@njcbw.org
- P.O. Box U, Hewitt, N.J. 07421
- HOTLINE: 800-SOS-9470 (800-767-9470)
- Office: 973-248-0776
- Email: info@sosdv.org
New Mexico
New Mexico State Coalition Against Domestic Violence
- 201 Coal Avenue SW, Albuquerque, NM 87102
- TOLL-FREE: 800-773-3645 (in New Mexico Only)
- Legal Helpline: 800-209-DVLH
- Phone: 505-246-9240
- FAX: 505-246-9434
- Email: info@nmcadv.org
New York
New York State Coalition Against Domestic Violence
- 350 New Scotland Avenue, Albany New York 12208
- Phone: 518-482-5465
- English: 1-800-942-6906
- English TTY: 1-800-818-0656
- Spanish: 1-800-942-6908
- Spanish TTY: 1-800-780-7660
- Fax: 518-482-3807
- Email us at nyscadv@nyscadv.org
North Carolina
North Carolina Coalition Against Domestic Violence
- 123 W. Main Street, Suite 700
- Durham, NC 27701
- Phone: 919-956-9124
- HOTLINE: 1-888-232-9124
- FAX: 919-682-1449
- Western Office:
- PO Box 17398, Asheville, NC 28816
- Phone: 828-505-3708
North Dakota
North Dakota Council on Abused Women's Services
- State Networking Office, 418 East Rosser Avenue, Suite 320, Bismarck, ND 58501
- TOLL-FREE: 888-255-6240 (In ND Only)
- Phone: 701-255-6240
- FAX: 701-255-1904
Ohio
Ohio Domestic Violence Network
- 4807 Evanswood Drive, Suite 201, Columbus, Ohio 43229
- Phone: 614-781-9651
- TTY: 614 781-9654
- HOTLINE: 800-934-9840
- Fax: 614 781-9652
- Email: info@odvn.org
Oklahoma
Oklahoma Coalition Against Domestic Violence and Sexual Assault
- 3815 N. Santa Fe Avenue, Suite 124, Oklahoma City, OK 73118
- Telephone: 405-524-0700
- Fax: 405-524-0711
- Email: info@ocadvsa.org
- Education Office:
- PO Box 135, Poteau, OK 74953
- Telephone: 918-647-5814
- Fax: 918-649-3772
Oregon
Oregon Coalition Against Domestic Violence and Sexual Assault
- State Office: 380 Spokane St., Suite 100, Portland, OR 97202
- Telephone: 503-230-1951
- TTY: 1-800-553-2508
- Fax: 503-230-1973
- Statewide Crisis Number: 1-888-235-5333
Pennsylvania
Pennsylvania Coalition Against Domestic Violence/National Resource Center on Domestic Violence
- 6440 Flank Drive, Suite 1300, Harrisburg, PA 17112-2778
- Phone: 717-545-6400
- Toll-Free: 800-932-4632
- TTY: 800-553-2508
- FAX: 717-671-8149
Women's Center of Montgomery County
- Main Administrative Office:
- 101 Washington Lane, Ste. WC-1, Jenkintown PA 19046
- Toll-free hotline: 1-800-773-2424
- Norristown Office:
- Women's Advocacy Project
- 400 Courthouse Plaza, 18 W. Airy St., Norristown PA 19404
- 610-279-1548
- Pottstown Office:
- Women's Advocacy Project
- 555 High Street, 2nd Floor, Pottstown PA 19464
- 610-970-7363
- Bryn Mawr Office:
- 610-525-1427
- Lansdale Office:
- 215-853-8060
- P.O. Box 764,Norristown, PA 19404
- Phone: 610-277-1860
- HOTLINE: 1-800-642-3150
- Fax: 610-277-64025
- E-Mail: LaurelHaus@aol.com
Rhode Island
Rhode Island Coalition Against Domestic Violence
- 422 Post Road, Suite 202, Warwick, RI 02888
- HOTLINE: 800-494-8100
- Phone: 401-467-9940
- FAX: 401-467-9943
- Email: ricadv@ricadv.org
South Carolina
South Carolina Coalition Against Domestic Violence & Sexual Assault
- P.O. Box 7776, Columbia, SC 29202-7776
- TOLL-FREE: 800-260-9293
- Phone: 803-256-2900
- FAX: 803-256-1030
South Dakota
South Dakota Coalition Against Domestic Violence and Sexual Assault
- P.O. Box 141, Pierre, SD 57501
- HOTLINE: 800-430-7233
- Phone: 605-945-0869
- FAX: 605-945-0870
- PO Box 1402, Sioux Falls, SD 57101
- (605) 271-3171 Phone
- (605) 271-3172 Fax
- 1-877-317-3096 (Info/Referral only)
- PO Box 41, 310 S. Kline St., Aberdeen, SD 57402-0041
- Phone: 605 226-1212
- Toll-Free: 888-290-2935
- Fax: 650-226-2430
- Email (general information only): safeharbor@safeharbor.ws
Tennessee
Tennessee Task Force Against Domestic Violence
- 2 International Plaza Dr., Suite 425, Nashville, TN 37217
- TOLL-FREE: 800-289-9018
- Phone: 615-386-9406
- FAX: 615-383-2967
- Email: webmistress@tcadsv.org
Texas
Texas Council on Family Violence
- P.O. Box 161810, Austin, TX 78716
- TOLL-FREE: 800-525-1978
- Phone: 512-794-1133
- FAX: 512-794-1199
- P.O. Box 25, Killeen, Texas 76540
- Phone: 254-773-7765
- Fax: 254-526-6111
Utah
Utah Domestic Violence Coalition
- 205 North 400 West, Salt Lake City, UT 84111-2178
- Phone: 800-897-5465
- FAX: 800-897-5465
- E-mail: admin@udvc.org
Vermont
- PO BOX 1535, Burlington, VT
- Phone: 802-658-3131
- HOTLINE: 802-658-1996
- TTY: 802-658-1996
- Toll-free: 1-800-228-7395
- E-mail: whbw@whbw.org
- Women's Rape Crisis Center; Vermont
- 24 Hour HOTLINE: 802-863-1236
- Statewide HOTLINE: 800-489-7273
Vermont Network Against Domestic Violence and Sexual Assault
- P.O. Box 405, Montpelier, VT 05601
- Phone: 802-223-1302
- TTY: 800-223-1115
- 24 Hour HOTLINE: 1 800 228 7395
- FAX: 802-223-6943
- E-mail: info@vtnetwork.org
Virginia
Virginians Family Violence and Sexual Assault Hotline
- Charlottesville, VA
- 302 Hickman Rd, Suite 101, Charlottesville, VA 22911
- Phone: 434-979-9002
- Fax: 434-979-9003
- Richmond, VA
- 5008 Monument Ave., Suite A, Richmond, VA 23230
- Phone: 804-377-0335
- Fax: 804-377-0339
- E-mail: info@vsdvalliance.org
Washington
Washington State Coalition Against Domestic Violence
- WSCADV- Olympia Office
- 711 Capitol Way, Suite 702, Olympia, WA 98501
- Phone: 360-586-1022
- Fax: 360-586-1024
- TTY: 360-586-1029
- WSCADV - Seattle Office
- 1402 - 3rd Ave, Suite 406, Seattle WA 98101
- 206-389-2515
- 206-389-2520 FAX
- 206- 389-2900 TTY
- E-mail: wscadv@wscadv.org
- Washington State Domestic Violence Hotline
- Tel: 800-562-6025
- E-mail: csn@willapabay.org
West Virginia
West Virginia Coalition Against Domestic Violence
- Elk Office Center, 5004 Elk River Road, Elkview, WV 25071
- Phone: 304-965-3552
- FAX: 304-965-3572
Wisconsin
Manitowoc County Domestic Violence Center
- 1127 S. 22nd. St, Manitowoc, WI 54220
- Phone: 920-684-5770
- HOTLINE: 877-275-6888
- Fax: 920-684-6344
- E-mail: dvc@sbcglobal.net
Wisconsin Coalition Against Domestic Violence
- 1400 E. Washington Ave. Suite 227, Madison, WI 53703
- Phone: 608-255-0539
- Fax: 608-255-3560
Wyoming
Wyoming Coalition Against Domestic Violence and Sexual Assault
- P.O. Box 236, 710 Garfield Street, Suite 218, Laramie, WY 82073
- TOLL-FREE: 800-990-3877
- Phone: 307-755-5481
- Legal Staff: 307-755-0992
- Fax: 307-755-5482
- E-mail: info@wyomingdvsa.org
YWCA Battered Women Task Force-Topeka
- 225 SW 12th St., Topeka, KS 66612
- Phone: 785-233-1750
- FAX: 785-233-4867
- 24 Hour HOTLINE: 1-888-822-2983
- E-mail: volunteer@ywcaneks.org
National Organizations
- 100 Montgomery Street, San Francisco, CA 94129
- Phone: 415-678-5500
- TTY: 866-678-8901
- FAX: 415-529-2930
- E-mail: info@futureswithoutviolence.org
National Coalition Against Domestic Violence
- Main Office: 1120, Lincoln Street Suite 1603, Denver, CO 80203
- Phone: 303 839 1852
- TTY: (303) 839-8459
- Fax: (303) 831-9251
- E-mail: mainoffice@ncadv.org
Public Policy Office
- 1633 Q Street NW, Suite 210, Washington, DC 20009
- Phone: (202) 745-1211
- TTY: (202) 745-2042
- Fax: (202) 745-0088
- E-mail: publicpolicy@ncadv.org
National Battered Women's Law Project
- 275 7th Avenue, Suite 1206, New York, NY 10001
- Phone: 212-741-9480
- FAX: 212-741-6438
- 2 Lafayette Street, 3rd Floor, New York, NY 10007
- Crime Victims HOTLINE: 800-621-4673
- Rape and Sexual Assult & Incest HOTLINE: 212-227-3000
- TYY (for all HOTLINES) 866-604-5350
- Fax: 212-577-3897
- E-mail: website@safehorizon.org
National Resource Center on Domestic Violence
- Pennsylvania Coalition Against Domestic Violence
- 6400 Flank Drive, Suite 1300, Harrisburg, PA 17112
- Phone: 800-537-2238
- Fax: 717-545-9456
- Legal Office:
- Phone: 717-545-6400
- TOLL-FREE: 800-932-4632
- TTY : 800-533-2508
- Fax: 717-671-5542
- National Resource Center on Domestic Violence
- Phone: 800-537-2238
- TTY: 888-Rx-ABUSE; 800- 595 -4889
- Fax: 717-545-9456
Battered Women's Justice Project
- Minnesota Program Development, Inc
- 1801 Nicollet Ave, Suite 102, Minneapolis, MN 55403
- Phone: 800-903-0111, ext.1
- Phone: 612-824-8768
- Fax: 612-824-8965
- E-mail: technicalassistance@bwjp.org
Resource Center on Domestic Violence, Child Protection, and Custody
- NCJFCJ
- P.O. Box 8970, Reno, NV 89507
- Office: 775-784-6012
- Phone: 800-527-3223
- Fax: 775-784-6628
- Email: staff@ncjfcj.org
Battered Women's Justice Project
- c/o National Clearinghouse for the Defense of Battered Women
- 125 South 9th Street, Suite 302, Philadelphia, PA 19107
- TOLL-FREE: 800-903-0111 ext. 3
- Phone: 215-351-0010
- FAX: 215-351-0779
National Clearinghouse is a national resource and advocacy center providing assistance to women defendants, their defense attorneys, and other members of their defense teams in an effort to ensure justice for battered women charged with crimes.
National Clearinghouse on Marital and Date Rape
- 2325 Oak Street, Berkeley, CA 94708
- Phone: 510-524-1582
- 2400 N. 45th Street #10, Seattle, WA 98103
- Phone: 206-634-1903, ext. 10
- Fax: 206-634-0115
- Email: info@faithtrustinstitute.org
National Network to End Domestic Violence
- 2001 S Street NW, Suite 400, Washington, DC 20009
- Phone: 202-543-5566
- HOTLINE: 800-799-SAFE (7233)
- TTY: 800-787-3224
- FAX: 202-543-5626
References
- Centers for Disease Control and Prevention. (CDC). (2020a). Intimate partner violence. Centers for Disease Control and Prevention. Retrieved September 25, 2021. Visit Source.
- Centers for Disease Control and Prevention. (CDC). (2020b). Preventing intimate partner violence. Centers for Disease Control and Prevention. Retrieved September 25, 2021. Visit Source.
- Centers for Disease Control and Prevention. (CDC). (2020c). Intimate partner violence, sexual violence, and stalking among men. Centers for Disease Control and Prevention. Retrieved May 18, 2022. Visit Source.
- Cline, D., Ma, O., Meckler, G., Stapczynski, J., Thomas, S., Tintinalli, J.., &; Yealy, D. (2020). Tintinalli's emergency medicine: A comprehensive study guide (9th ed.). McGraw-Hill Education. Visit Source.
- DeCapua, M. (2017). Domestic Violence, Sexual Violence, Intimate Partner Violence. Visit Source.
- DomesticShelters.org. (2016). Women as the abusers. DomesticShelters.org. Visit Source.
- Kippert, A. (2021). A guide for male survivors of domestic violence. DomesticShelters.org. Visit Source.
- Resnick, A. (2021). Domestic violence in the LGBTQ+ community. Verywellmind.com. Visit Source.
- Sadock, B., Boland, R., Verduin, M., & Ruiz, P. (2021). Kaplan & Sadock's Synopsis of Psychiatry (12th ed.). Wolters Kluwer. Visit Source.
- U.S. Department of Health and Human Services. (2010). Compendium of state statutes and policies on domestic violence and healthcare. Family Violence Prevention Fund. Retrieved September 26, 2021. Visit Source.
- World Health Organization. (WHO). (2021). Violence against women. World Health Organization. Retrieved September 25, 2021. Visit Source.